|
Hace más de 60 años, legisladores en Colorado adoptaron la idea de que la intervención temprana podría prevenir el abuso infantil y salvar vidas. El requisito del estado de que ciertos profesionales informaran a las autoridades cuando sospechaban que un niño había sido maltratado o descuidado fue una de las primeras leyes de informes obligatorios en la nación. Desde entonces, estas leyes se han expandido a nivel nacional para abarcar más tipos de maltrato, incluido el abandono, que ahora representa la mayoría de los informes, y han aumentado el número de profesiones obligadas a informar. En algunos estados, se requiere que todos los adultos informen lo que sospechan que pueda ser un caso de abuso o negligencia. Pero ahora hay esfuerzos en Colorado y otros estados para revertir estas leyes, argumentando que el resultado ha sido demasiados informes infundados, que perjudican desproporcionadamente a las familias que son pobres, negras, indígenas o tienen miembros con discapacidades. “Hay una larga y deprimente historia basada en el enfoque de que nuestra respuesta principal a una familia en dificultades es reportar”, dijo Mical Raz, médica e historiadora de la Universidad de Rochester en Nueva York. “Ahora hay una gran cantidad de evidencia que demuestra que más informes no están asociados con mejores resultados para los niños”. Stephanie Villafuerte, defensora del pueblo para la protección infantil de Colorado, supervisa un grupo de trabajo para reexaminar las leyes de informes obligatorios del estado. Dijo que el grupo busca equilibrar la necesidad de informar casos legítimos de abuso y negligencia con el deseo de eliminar informes inapropiados. “Esto está diseñado para ayudar a las personas que se ven afectadas de manera desproporcionada”, dijo Villafuerte. “Espero que la combinación de estos esfuerzos pueda marcar la diferencia”. A algunos críticos les preocupa que los cambios a la ley pueda dar lugar a que se pasen por alto casos de abuso. Los trabajadores médicos y de cuidado infantil que forman parte del grupo de trabajo han expresado preocupación sobre la responsabilidad legal. Aunque es raro que las personas sean acusadas penalmente por no informar, también pueden enfrentar responsabilidad civil o repercusiones profesionales, incluidas amenazas a sus licencias. El ser reportado a los servicios de protección infantil se está volviendo cada vez más común. Más de 1 de cada 3 niños en el país será objeto de una investigación de abuso y negligencia infantil para cuando cumplan 18 años, según una estimación que se cita con frecuencia, un estudio de 2017 financiado por la Oficina de Niños del Departamento de Salud y Servicios Humanos. A las familias negras y nativas americanas, las familias pobres y los padres o niños con discapacidades se las mira con lupa. La investigación ha encontrado que, entre estos grupos, los padres tienen más probabilidades de perder los derechos parentales y los niños tienen más probabilidades de terminar en hogares temporales. En una abrumadora mayoría de investigaciones, no se confirma ningún abuso o negligencia. Sin embargo, los que estudian cómo afectan estas investigaciones a las familias las describen como aterradoras y aislantes. En Colorado, el número de informes de abuso y negligencia infantil ha aumentado un 42% en la última década, y alcanzó un récord de 117,762 el año pasado, según datos estatales. Aproximadamente, otras 100,000 llamadas a la línea directa no se contaron como informes porque eran solicitudes de información o se referían a asuntos como la manutención de los hijos o la protección de adultos, dijeron oficiales del Departamento de Servicios Humanos de Colorado. El aumento de los informes se puede rastrear hasta una política que alienta a una amplia gama de profesionales —incluidos el personal escolar y médico, terapeutas, entrenadores, miembros del clero, bomberos, veterinarios, dentistas y trabajadores sociales— a llamar a una línea directa cada vez que tengan una preocupación. Estas llamadas no reflejan un aumento en el maltrato. Más de dos tercios de los informes que reciben las agencias en Colorado se desestiman porque no cumplen con el umbral para la investigación. De los niños cuyos casos se evalúan, se comprueba que el 21% ha sufrido abuso o negligencia. El número real de casos confirmados no ha aumentado en la última década. Si bien los estudios no demuestran que las leyes que obligan a informar mantengan seguros a los niños, informó el grupo de trabajo de Colorado en enero, hay evidencia de daño. “El informe obligatorio impacta desproporcionadamente a las familias de color”, iniciando el contacto entre los servicios de protección infantil y familias que no presentan preocupaciones por abuso o negligencia, dijo el grupo de trabajo. Este grupo también está analizando si una mejor selección podría mitigar “el impacto desproporcionado del informe obligatorio en comunidades con recursos limitados, comunidades de color y personas con discapacidades”. También señaló que la única forma de informar preocupaciones sobre un niño es con un informe formal a una línea directa. Sin embargo, muchas de esas llamadas no son para informar sobre abuso en absoluto, sino intentos de conectar a niños y familias con recursos como alimentos o asistencia para la vivienda. Los que llaman a la línea directa pueden querer ayudar, pero las familias que son objeto de informes erróneos de abuso y negligencia rara vez lo ven de esa manera. Esto incluye a Meighen Lovelace, que vive en una zona rural de Colorado y que pidió a KFF Health News que no revelara su ciudad natal por temor a atraer la atención no deseada de funcionarios locales. Para la hija de Lovelace, que es neurodivergente y tiene discapacidades físicas, los informes comenzaron en 2015, cuando empezó el preescolar a los 4 años. Los maestros y proveedores médicos que hacían los informes a menudo sugerían que la agencia de servicios humanos del condado podría ayudar a la familia de Lovelace. Pero las investigaciones que siguieron fueron invasivas y traumáticas. “Nuestro mayor temor latente es, ‘¿van a llevarse a nuestros hijos?'”, dijo Lovelace, quien es defensora de la Colorado Cross-Disability Coalition, una organización que aboga por los derechos civiles de las personas con discapacidades. “Tenemos miedo de pedir ayuda. Nos está impidiendo ingresar a los servicios debido al miedo al bienestar infantil”, expresó. Funcionarios de servicios humanos, estatales y del condado, dijeron que no podían comentar sobre casos específicos. El grupo de trabajo de Colorado planea sugerir aclarar las definiciones de abuso y negligencia bajo la ley de informe obligatorio del estado. Los que tienen que informar no deben “hacer un informe únicamente debido a la raza, clase o género de una familia/niño”, ni debido a una vivienda, muebles, ingresos o ropa inadecuados. Además, no debe haber un informe basado únicamente en el “estado de discapacidad del menor, padre o tutor”, según la recomendación preliminar del grupo. También planean recomendar capacitación adicional para los que tienen la obligación de informar, ayuda para profesionales que están decidiendo si hacer una llamada o no, y un número de teléfono alternativo, o “línea directa cálida”, para casos en los que los que llaman creen que una familia necesita ayuda material, en lugar de vigilancia. Los críticos dicen que estos cambios podrían dejar a más niños vulnerables a abusos no denunciados. “Me preocupa que agregando sistemas como la línea directa cálida, se nos escabullan los casos en lo que los niños están en verdadero peligro, y que no reciban ayuda”, dijo Hollynd Hoskins, abogada que representa a víctimas de abuso infantil. Hoskins ha demandado a profesionales que no informan sus sospechas. El grupo de trabajo de Colorado incluye a funcionarios de salud y educación, fiscales, defensores de las víctimas, representantes del bienestar infantil del condado y abogados, así como a cinco personas que tienen experiencia en el sistema de bienestar infantil. Planea finalizar sus recomendaciones a principios del próximo año con la esperanza de que los legisladores estatales consideren cambios en la política en 2025. La implementación de cualquier nueva ley podría llevar varios años. Colorado es uno de varios estados, incluidos Nueva York y California, que han considerado recientemente cambios para restringir, en lugar de expandir, el informe sobre supuestos abusos. En la ciudad de Nueva York, se está capacitando a los maestros para que lo piensen dos veces antes de hacer un informe, mientras que el estado de Nueva York introdujo una “línea directa cálida” para ayudar a conectar a las familias con recursos como vivienda y cuidado infantil. En California, un grupo de trabajo estatal destinado a cambiar del “informe obligatorio al apoyo comunitario” está planeando recomendaciones similares a las de Colorado. Entre los que abogan por el cambio están las personas con experiencia en el sistema de bienestar infantil. Incluyen a Maleeka Jihad, quien lidera la Coalición MJCF con sede en Denver, que aboga por la abolición del informe obligatorio junto con el resto del sistema de bienestar infantil, citando su daño a las comunidades negras, nativas americanas y latinas. “El informe obligatorio es otra forma de mantenernos vigilados por blancos [no hispanos]”, dijo Jihad. A él mismo cuando era niño lo arrebataron del cuidado de un padre amoroso y lo colocaron en el sistema temporal. La reforma no es suficiente, dijo. “Sabemos lo que necesitamos, y generalmente son fondos y recursos”. Algunos de estos recursos —como vivienda asequible y cuidado infantil— no existen a un nivel suficiente para todas las familias de Colorado que los necesitan, dijo Jihad. Otros servicios están disponibles, pero hay que encontrarlos. Lovelace dijo que los informes disminuyeron después que la familia obtuvo la ayuda que necesitaba, en forma de una exención de Medicaid que pagaba por atención especializada para las discapacidades de su hija. Ahora, la niña está en séptimo grado y le va bien. Ninguno de los trabajadores sociales que visitaron a la familia mencionó la exención, dijo Lovelace. “Realmente creo que no sabían nada al respecto”. KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF. USE OUR CONTENTThis story can be republished for free (details). from https://ift.tt/Yz1mDqb Check out http://plush-draw15.tumblr.com/
0 Comments
Una mañana de enero de 2021, Carol Rosen recibió un tratamiento estándar para el cáncer de mama metastásico. Murió después de tres semanas de sufrimiento, con un dolor insoportable causado por la misma droga que debería haber ayudado a prolongar su vida. Rosen, maestra jubilada de 70 años, pasó sus últimos días angustiada, sufriendo de diarrea intensa, náuseas y dolorosas llagas en la boca que le impedían comer, beber y, finalmente, hablar. La piel se le desprendía del cuerpo. Sus riñones y su hígado habían dejado de funcionar. “Tu cuerpo arde desde”, dijo la hija de Rosen, Lindsay Murray, de Andover, Massachusetts. Rosen fue una de los más de 275,000 pacientes con cáncer en los Estados Unidos a quienes cada año se les administra fluorouracilo, también conocido como 5-FU, o que toman un medicamento casi idéntico en forma de pastilla llamado capecitabina, como ella lo hacía. Estos tipos de quimioterapia comunes son difíciles de tolerar en general, pero para los pacientes que tienen deficiencia de una enzima que metaboliza la droga, puede ser una tortura o causar la muerte. La toxicidad por fluorouracilo ocurre porque los medicamentos permanecen en el cuerpo durante horas en vez de ser metabolizados y excretados rápidamente. Se estima que las drogas matan a 1 de cada 1,000 pacientes que las toman --cientos de personas cada año— y hacen que 1 de cada 50 pacientes se enfermen gravemente o deban ser internados. Los médicos pueden realizar pruebas para detectar la deficiencia y obtener resultados en una semana, y así determinar si cambiar de medicamento o reducir la dosis para los pacientes que tienen la variante genética asociada con el riesgo. Sin embargo, una encuesta reciente encontró que sólo el 3% de los oncólogos piden las pruebas de forma habitual antes de administrar 5-FU o capecitabina a sus pacientes. Esto se debe a que las pautas de tratamiento del cáncer más aceptadas en el país, emitidas por la Red Nacional Integral del Cáncer, no recomiendan las pruebas de manera preventiva. La Administración de Alimentos y Medicamentos (FDA) agregó nuevas advertencias sobre los riesgos letales del 5-FU a la etiqueta del medicamento el 21 de marzo pasado, después de consultas de KFF Health News sobre la política de la agencia con respecto a la droga. Sin embargo, no exigió que los médicos realicen la prueba antes de recetar tratamientos de quimioterapia. La agencia, cuyo plan para reforzar la supervisión de las pruebas de laboratorio fue abordado en una audiencia en la Cámara de Representantes, también el 21 de marzo, dijo que no podía recomendar las pruebas de toxicidad del 5-FU porque nunca las había revisado. Pero actualmente la FDA no revisa la mayoría de las pruebas de diagnóstico, dijo Daniel Hertz, profesor asociado de la Escuela de Farmacia de la Universidad de Michigan. Durante años, Hertz, junto con otros médicos y farmacéuticos, ha solicitado a la FDA que agregue la máxima advertencia (llamada “caja negra”) a la etiqueta del medicamento, para instar a los profesionales que lo recetan a realizar las pruebas para detectar la deficiencia de la enzima. “La FDA tiene la responsabilidad de asegurar que los medicamentos se utilicen de forma segura y eficaz”, dijo. La falta de esta advertencia, afirmó, “es una abdicación de su responsabilidad”. Las nuevas advertencias son “un pequeño paso adelante, pero no el cambio radical que necesitamos”, afirmó. Europa lidera en seguridad Las autoridades farmacéuticas británicas y de la Unión Europea recomiendan la prueba desde 2020. En Estados Unidos, un número pequeño pero creciente de hospitales, grupos profesionales y defensores de la salud, incluyendo la Sociedad Americana del Cáncer, también recomiendan las pruebas de forma rutinaria. La mayoría de las aseguradoras estadounidenses, tanto públicas como privadas, cubren las pruebas, que Medicare reembolsa por $175, aunque pueden costar más dependiendo de cuántas variantes detectan. En sus últimas directrices sobre el cáncer de colon, el panel de la Red Nacional Integral del Cáncer señaló que no todas las personas que portan la variante genética se enferman cuando toman el medicamento, y que recetar dosis más bajas para estos pacientes podría privarlos de curarse o de tener una remisión del cáncer. Muchos médicos del panel, incluyendo Wells Messersmith, oncólogo de la Universidad de Colorado, dijeron que nunca han registrado una muerte por 5-FU. 
En los hospitales europeos, se empieza con la mitad o un cuarto de la dosis de 5-FU para los pacientes cuyas pruebas muestran que metabolizan la droga lentamente. Luego, se aumenta la dosis si el paciente responde bien al medicamento. Los defensores de este abordaje dicen que las autoridades estadounidenses de oncología están demorando el tratamiento innecesariamente, y perjudicando a las personas. “Creo que se trata de una terquedad de parte de las personas que participan en estos paneles”, dijo Gabriel Brooks, oncólogo e investigador del Dartmouth Cancer Center. “Piensan: ‘Somos oncólogos, los medicamentos son nuestras herramientas, no queremos buscar razones para no usar nuestras herramientas’”. Los oncólogos están acostumbrados a la toxicidad de la quimioterapia y tienden a tener una actitud de “sin dolor no hay recompensa”, dijo. El 5-FU se utiliza desde la década de 1950. Por otro lado, “cualquiera que haya perdido un paciente de esta manera va a querer someter a todos a las pruebas”, dijo Robert Diasio, de la Clínica Mayo, quien ayudó a realizar importantes estudios sobre la deficiencia genética en 1988. Muchos oncólogos utilizan las pruebas genéticas para determinar cuál de los costosos medicamentos disponibles usar para reducir el tamaño de un tumor. Pero no siempre sucede lo mismo con las pruebas genéticas destinadas a mejorar la seguridad de los medicamentos, dijo Mark Fleury, director de políticas de Cancer Action Network, una organización defensora sin fines de lucro de la Sociedad Americana del Cáncer. En el caso de medicamentos nuevos, cuando se trata de pruebas para determinar si son apropiados para cada paciente, “hay muchas más fuerzas alineadas para que se realicen estas pruebas”, dijo Fleury. “Pero estas fuerzas y grupos interesados no están involucrados” con una droga genérica como el 5-FU, que fue aprobada por primera vez en 1962 y cuesta aproximadamente $17 por mes. Carol Rosen fue una de más de 1,000 pacientes tratadas con fluoropirimidina en 2021. Su hija estaba desconsolada y furiosa después de la muerte de Rosen. “Quería demandar al hospital. Quería demandar al oncólogo”, dijo Murray. “Pero me di cuenta que eso no era lo que mi mamá hubiera querido”. Le escribió al director de control de calidad del Dana-Farber, Joe Jacobson, para instarlo a realizar las pruebas de forma rutinaria. Jacobson respondió el mismo día, y el hospital adoptó rápidamente un sistema de pruebas que ahora cubre a más del 90% de los pacientes que podrían ser tratados con fluoropirimidina. Se detectaron alrededor de 50 pacientes con variantes de riesgo en los primeros 10 meses, dijo Jacobson. Dana-Farber utiliza una prueba de la Clínica Mayo que detecta ocho variantes potencialmente riesgosas del gen. Los hospitales de Veterans Affairs utilizan una prueba que detecta 11 variantes, mientras que la mayoría de los demás identifican sólo cuatro variantes. Distintas pruebas para distintas ascendencias Cuantas más variantes detecte una prueba, mejores son las posibilidades de encontrar variantes genéticas menos comunes en poblaciones étnicamente diversas. Por ejemplo, las deficiencias más peligrosas en personas de ascendencia africana y europea, respectivamente, son causadas por distintas variantes. Hay pruebas que pueden identificar cientos de variantes que afectan el metabolismo de la droga, pero tardan más y son más caras. Estas son tristes realidades para Scott Kapoor, un médico de urgencias que vive cerca de Toronto cuyo hermano, Anil Kapoor, murió en febrero de 2023 de toxicidad por 5-FU. Anil Kapoor era un conocido urólogo y cirujano, investigador, médico y un amigo divertido: a su funeral fueron cientos de personas. Su muerte a los 58 años, unas pocas semanas después que le diagnosticaran cáncer de colon en estadio 4, sorprendió y enfureció a su familia. El sistema de salud de Ontario, donde se trató Kapoor, recién había empezado a realizar pruebas para detectar cuatro variantes genéticas, identificadas por estudios desarrollados en poblaciones principalmente europeas. Anil Kapoor y sus hermanos, hijos de inmigrantes de la India nacidos en Canadá, son portadores de una variante genética que parece estar asociada con las personas de ascendencia del sur de Asia. Scott Kapoor apoya pruebas más extensas para detectar la mutación, ya que sólo alrededor de la mitad de los habitantes de Toronto son de ascendencia europea, y sostiene que el antídoto contra la toxicidad por fluoropirimidina, aprobado por la FDA en 2015, debería estar fácilmente disponible. Sin embargo, este antídoto sólo funciona por unos días después del consumo del fármaco, y los síntomas definitivos suelen tardar más tiempo en aparecer. Lo más importante, dijo, es que los pacientes estén al tanto del riesgo. “Les dices: ‘Te voy a dar un medicamento que tiene una probabilidad de 1 entre 1,000 de matarte. Puedes hacerte esta prueba’. La mayoría de los pacientes dirán: ‘Quiero hacerme esa prueba y la pagaré’, o simplemente: ‘Reduzca la dosis a la mitad’”. Murray percibe un impulso por las pruebas obligatorias. En 2022, la Universidad de Ciencias y Salud de Oregon pagó $1 millón para resolver una demanda tras una muerte por sobredosis. “Lo que va a romper esa barrera son las demandas y las grandes instituciones como Dana-Farber que están implementando programas y viendo cómo tienen éxito”, dijo. “Creo que los proveedores se sentirán acorralados. Van a seguir escuchando a las familias y tendrán que hacer algo al respecto”. KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF. USE OUR CONTENTThis story can be republished for free (details). from https://ift.tt/Xf8tVjw Check out http://plush-draw15.tumblr.com/ Monica Kelly was thrilled to learn she was expecting her second child. The Tennessee mother was around 13 weeks pregnant when, according to a lawsuit filed against the state of Tennessee, doctors gave her the devastating news that her baby had Patau syndrome. The genetic disorder causes serious developmental defects and often results in miscarriage, stillbirth, or death within one year of birth. Continuing her pregnancy, doctors told her, could put her at risk of infection and complications that include high blood pressure, organ failure, and death. But they said they could not perform an abortion due to a Tennessee law banning most abortions that went into effect two months after the repeal of Roe v. Wade in June 2022, court records show. So Kelly traveled to a northwestern Florida hospital to get an abortion while about 15 weeks pregnant. She is one of seven women and two doctors suing Tennessee because they say the state’s near-total abortion ban imperils the lives of pregnant women. More than 25,000 women like Kelly traveled to Florida for an abortion over the past five years, state data shows. Most came from states such as Alabama, Louisiana, and Mississippi with little or no access to abortion, data from the Centers for Disease Control and Prevention shows. Hundreds traveled from as far as Texas. But a recent Florida Supreme Court ruling paved the way for the Sunshine State to enforce a six-week ban beginning in May, effectively leaving women in much of the South with little or no access to abortion clinics. The ban could be short-lived if 60% of Florida voters in November approve a constitutional amendment adding the right to an abortion.  Related Coverage Related Coverage
Conservative Justices Stir Trouble for Republican Politicians on AbortionRead MoreIn the meantime, nonprofit groups are warning they may not be able to meet the increased demand for help from women from Florida and other Southeastern states to travel for an abortion. They fear women who lack the resources will be forced to carry unwanted pregnancies to term because they cannot afford to travel to states where abortions are more available. That could include women whose pregnancies, like Kelly’s, put them at risk. “The six-week ban is really a problem not just for Florida but the entire Southeast,” said McKenna Kelley, a board member of the Tampa Bay Abortion Fund. “Florida was the last man standing in the Southeast for abortion access.” Travel Bans and Stricter Limits Supporters of the Florida restrictions aren’t backing down. Some want even stricter limits. Republican state Rep. Mike Beltran voted for both the 15-week and six-week bans. He said the vast majority of abortions are elective and that those related to medical complications make up a tiny fraction. State data shows that 95% of abortions last year were either elective or performed due to social or economic reasons. More than 5% were related to issues with either the health of the mother or the fetus. Beltran said he would support a ban on travel for abortions but knows it would be challenged in the courts. He would support measures that prevent employers from paying for workers to travel for abortions and such costs being tax-deductible, he said. “I don’t think we should make it easier for people to travel for abortion,” he said. “We should put things in to prevent circumvention of the law.” Both abortion bans were also supported by GOP state lawmaker Joel Rudman. As a physician, Rudman said, he has delivered more than 100 babies and sees nothing in the current law that sacrifices patient safety. “It is a good commonsense law that provides reasonable exceptions yet respects the sanctity of life for both mother and child,” he said in a text message. Last year, the first full year that many Southern states had bans in place, more than 7,700 women traveled to Florida for an abortion, an increase of roughly 59% compared with three years ago. The Tampa Bay Abortion Fund, which is focused on helping local women, found itself assisting an influx of women from Arkansas, Georgia, Mississippi, Louisiana, and other states, Kelley said. In 2023, it paid out more than $650,000 for appointment costs and over $67,000 in other expenses such as airplane tickets and lodging. Most of those who seek assistance are from low-income families including minorities or disabled people, Kelley said. “We ask each person, ‘What can you contribute?’” she said. “Some say zero and that’s fine.” Florida’s new law will mean her group will have to pivot again. The focus will now be on helping people seeking abortions travel to other states. But the destinations are farther and more expensive. Most women, she predicted, will head to New York, Illinois, or Washington, D.C. Clinic appointments in those states are often more expensive. The extra travel distance will mean help is needed with hotels and airfare. North Carolina, which allows abortions through about 12 weeks of pregnancy, may be a slightly cheaper option for some women whose pregnancies are not as far along, she said. Keeping up with that need is a concern, she said. Donations to the group soared to $755,000 in 2022, which Kelley described as “rage donations” made after the U.S. Supreme Court ended half a century of guaranteeing the federal right to an abortion. The anger didn’t last. Donations in 2023 declined to $272,000, she said. “We’re going to have huge problems on our hands in a few weeks,” she said. “A lot of people who need an abortion are not going to be able to access one. That’s really scary and sad.” Gray Areas Lead to Confusion The Chicago Abortion Fund is expecting that many women from Southeastern states will head its way. Illinois offers abortions up until fetal viability — around 24 to 26 weeks. The state five years ago repealed its law requiring parents to be notified when their children seek an abortion. About 3 in 10 abortions performed in Illinois two years ago — almost 17,000 — involved out-of-state residents, up from fewer than a quarter the previous year, according to state records. The Chicago nonprofit has prided itself on not turning away requests for help over the past five years, said Qudsiyyah Shariyf, a deputy director. It is adding staffers, including Spanish-language speakers, to cope with an anticipated uptick in calls for help from Southern states. She hopes Florida voters will make the crisis short-lived. “We’re estimating we’ll need an additional $100,000 a month to meet that influx of folks from Florida and the South,” she said. “We know it’s going to be a really hard eight months until something potentially changes.” Losing access to abortion, especially among vulnerable groups like pregnant teenagers and women with pregnancy complications, could also increase cases of mental illness such as depression, anxiety, and even post-traumatic stress disorder, said Silvia Kaminsky, a licensed marriage and family therapist in Miami.  related coverage related coverage
Can a Fetus Be an Employee? States Are Testing the Boundaries of Personhood After ‘Dobbs’Read MoreKaminsky, who serves as board president of the American Association for Marriage and Family Therapy, said the group has received calls from therapists seeking legal guidance about whether they can help a client who wants to travel for an abortion. That’s especially true in states such as Alabama, Georgia, and Missouri that have passed laws granting “personhood” status to fetuses. Therapists in many states, including Florida, are required to report a client who intends to harm another individual. “It’s creating all these gray areas that we didn’t have to deal with before,” Kaminsky said. Deborah Dorbert of Lakeland, Florida, said that Florida's 15-week abortion limit put her health at risk and that she was forced to carry to term a baby with no chance of survival. Her unborn child was diagnosed with Potter syndrome in November 2022. An ultrasound taken at 23 weeks of pregnancy showed that the fetus had not developed enough amniotic fluid and that its kidneys were undeveloped. Doctors told her that her child would not survive outside the womb and that there was a high risk of a stillbirth and, for her, preeclampsia, a pregnancy complication that can result in high blood pressure, organ failure, and death. One option doctors suggested was a pre-term inducement, essentially an abortion, Dorbert said. Dorbert and her husband were heartbroken. They decided an abortion was their safest option. 
At Lakeland Regional Health, she said, she was told her surgery would have to be approved by the hospital administration and its lawyers since Florida had that year enacted its 15-week abortion restriction. Florida’s abortion law includes an exemption if two physicians certify in writing that a fetus has a fatal fetal abnormality and has not reached viability. But a month elapsed before she got an answer in her case. Her doctor told her the hospital did not feel they could legally perform the procedure and that she would have to carry the baby to term, Dorbert said. Lakeland Regional Health did not respond to repeated calls and emails seeking comment. Dorbert’s gynecologist had mentioned to her that some women traveled for an abortion. But Dorbert said she could not afford the trip and was concerned she might break the law by going out of state. At 37 weeks, doctors agreed to induce Dorbert. She checked into Lakeland Regional Hospital in March 2023 and, after a long and painful labor, gave birth to a boy named Milo. “When he was born, he was blue; he didn’t open his eyes; he didn’t cry,” she said. “The only sound you heard was him gasping for air every so often.” She and her husband took turns holding Milo. They read him a book about a mother polar bear who tells her cub she will always love them. They sang Bob Marley and The Wailers’ “Three Little Birds” to Milo with its chorus that “every little thing is gonna be alright.” Milo died in his mother’s arms 93 minutes after being born. One year later, Dorbert is still dealing with the anguish. The grief is still “heavy” some days, she said. She and her husband have discussed trying for another child, but Florida’s abortion laws have made her wary of another pregnancy with complications. “It makes you angry and frustrated. I could not get the health care I needed and that my doctors advised for me,” she said. "I know I can’t go through what I went through again.” KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF. USE OUR CONTENTThis story can be republished for free (details). from https://ift.tt/HpKAuPv Check out http://plush-draw15.tumblr.com/ As a young GI at Fort Ord in Monterey County, California, Dean Osborn spent much of his time in the oceanside woodlands, training on soil and guzzling water from streams and aquifers now known to be contaminated with cancer-causing pollutants. “They were marching the snot out of us,” he said, recalling his year and a half stationed on the base, from 1979 to 1980. He also remembers, not so fondly, the poison oak pervasive across the 28,000-acre installation that closed in 1994. He went on sick call at least three times because of the overwhelmingly itchy rash. Mounting evidence shows that as far back as the 1950s, in an effort to kill the ubiquitous poison oak and other weeds at the Army base, the military experimented with and sprayed the powerful herbicide combination known colloquially as Agent Orange. While the U.S. military used the herbicide to defoliate the dense jungles of Vietnam and adjoining countries, it was contaminating the land and waters of coastal California with the same chemicals, according to documents. The Defense Department has publicly acknowledged that during the Vietnam War era it stored Agent Orange at the Naval Construction Battalion Center in Gulfport, Mississippi, and the former Kelly Air Force Base in Texas, and tested it at Florida’s Eglin Air Force Base. According to the Government Accountability Office, however, the Pentagon’s list of sites where herbicides were tested went more than a decade without being updated and lacked specificity. GAO analysts described the list in 2018 as “inaccurate and incomplete.” Fort Ord was not included. It is among about four dozen bases that the government has excluded but where Pat Elder, an environmental activist, said he has documented the use or storage of Agent Orange. According to a 1956 article in the journal The Military Engineer, the use of Agent Orange herbicides at Fort Ord led to a “drastic reduction in trainee dermatitis casualties.” “In training areas, such as Fort Ord, where poison oak has been extremely troublesome to military personnel, a well-organized chemical war has been waged against this woody plant pest,” the article noted. Other documents, including a report by an Army agronomist as well as documents related to hazardous material cleanups, point to the use of Agent Orange at the sprawling base that 1.5 million service members cycled through from 1917 to 1994. ‘The Most Toxic Chemical’ Agent Orange is a 50-50 mixture of two ingredients, known as 2,4-D and 2,4,5-T. Herbicides with the same chemical structure slightly modified were available off the shelf, sold commercially in massive amounts, and used at practically every base in the U.S., said Gerson Smoger, a lawyer who argued before the Supreme Court for Vietnam veterans to have the right to sue Agent Orange manufacturers. The combo was also used by farmers, forest workers, and other civilians across the country. The chemical 2,4,5-T contains the dioxin 2,3,7,8-tetrachlorodibenzo-p-dioxin or TCDD, a known carcinogen linked to several cancers, chronic conditions and birth defects. A recent Brown University study tied Agent Orange exposure to brain tissue damage similar to that caused by Alzheimer’s. Acknowledging its harm to human health, the Environmental Protection Agency banned the use of 2,4,5-T in the U.S. in 1979. Still, the other weed killer, 2,4-D is sold off-the-shelf today. “The bottom line is TCDD is the most toxic chemical that man has ever made,” Smoger said. 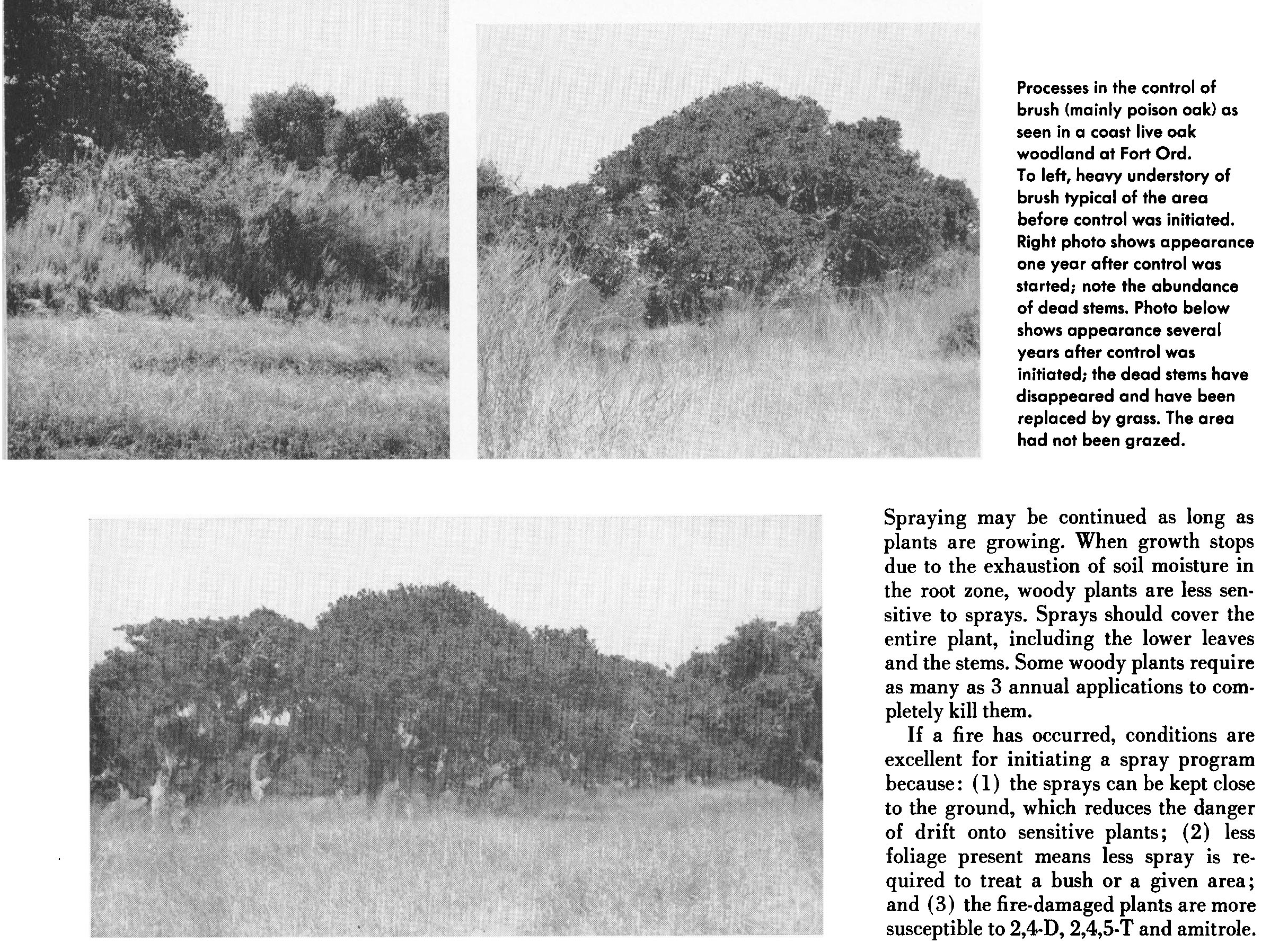
For years, the Department of Veteran Affairs has provided vets who served in Vietnam disability compensation for diseases considered to be connected to exposure to Agent Orange for military use from 1962 to 1975. Decades after Osborn’s military service, the 68-year-old veteran, who never served in Vietnam, has battled one health crisis after another: a spot on his left lung and kidney, hypothyroidism, and prostate cancer, an illness that has been tied to Agent Orange exposure. He says many of his old buddies from Fort Ord are sick as well. “Now we have cancers that we didn’t deserve,” Osborn said. The VA considers prostate cancer a “presumptive condition” for Agent Orange disability compensation, acknowledging that those who served in specific locations were likely exposed and that their illnesses are tied to their military service. The designation expedites affected veterans’ claims. But when Osborn requested his benefits, he was denied. The letter said the cancer was “more likely due to your age,” not military service. “This didn’t happen because of my age. This is happening because we were stationed in the places that were being sprayed and contaminated,” he said. Studies show that diseases caused by environmental factors can take years to emerge. And to make things more perplexing for veterans stationed at Fort Ord, contamination from other harmful chemicals, like the industrial cleaner trichloroethylene, have been well documented on the former base, landing it on the EPA’s Superfund site list in 1990. “We typically expect to see the effect years down the line,” said Lawrence Liu, a doctor at City of Hope Comprehensive Cancer Center who has studied Agent Orange. “Carcinogens have additive effects.” In February, the VA proposed a rule that for the first time would allow compensation to veterans for Agent Orange exposure at 17 U.S. bases in a dozen states where the herbicide was tested, used, or stored. Fort Ord is not on that list either, because the VA’s list is based on the Defense Department’s 2019 update. “It’s a very tricky question,” Smoger said, emphasizing how widely the herbicides were used both at military bases and by civilians for similar purposes. “On one hand, we were service. We were exposed. On the other hand, why are you different from the people across the road that are privately using it?” The VA says that it based its proposed rule on information provided by the Defense Department. “DoD’s review found no documentation of herbicide use, testing or storage at Fort Ord. Therefore, VA does not have sufficient evidence to extend a presumption of exposure to herbicides based on service at Fort Ord at this time,” VA press secretary Terrence Hayes said in an email. The Documentation Yet environmental activist Elder, with help from toxic and remediation specialist Denise Trabbic-Pointer and former VA physician Kyle Horton, compiled seven documents showing otherwise. They include a journal article, the agronomist report, and cleanup-related documents as recent as 1995 — all pointing to widespread herbicide use and experimentation as well as lasting contamination at the base. Though the documents do not call the herbicide by its colorful nickname, they routinely cite the combination of 2,4-D and 2,4,5-T. A “hazardous waste minimization assessment” dated 1991 reported 80,000 pounds of herbicides used annually at Fort Ord. It separately lists 2,4,5-T as a product for which “substitutions are necessary to minimize the environmental impacts.” The poison oak “control program” started in 1951, according to a report by Army agronomist Floyd Otter, four years before the U.S. deepened its involvement in Vietnam. Otter detailed the use of these chemicals alone and in combination with diesel oil or other compounds, at rates generally between “one to two gallons of liquid herbicide” per acre. “In conclusion, we are fairly well satisfied with the methods,” Otter wrote, noting he was interested in “any way in which costs can be lowered or quicker kill obtained.” An article published in California Agriculture more than a decade later includes before and after photos showing the effectiveness of chemical brush control used in a live-oak woodland at Fort Ord, again citing both chemicals in Agent Orange. The Defense Department did not respond to questions sent April 10 about the contamination or say when the Army stopped using 2,4,5-T at Fort Ord. “What’s most compelling about Fort Ord is it was actually used for the same purpose it was used for in Vietnam — to kill plants — not just storing it,” said Julie Akey, a former Army linguist who worked at the base in the 1990s and later developed the rare blood cancer multiple myeloma. Akey, who also worked with Elder, runs a Facebook group and keeps a list of people stationed on the base who later were diagnosed with cancer and other illnesses. So far, she has tallied more than 1,400 former Fort Ord residents who became sick. Elder’s findings have galvanized the group to speak up during a public comment period for the VA’s proposed rule. Of 546 comments, 67 are from veterans and others urging the inclusion of Fort Ord. Hundreds of others have written in regarding the use of Agent Orange and other chemicals at their bases. 
While the herbicide itself sticks around for only a short time, the contaminant TCDD can linger in sediment for decades, said Kenneth Olson, a professor emeritus of soil science at the University of Illinois Urbana-Champaign. A 1995 report from the Army’s Sacramento Corps of Engineers, which documented chemicals detected in the soil at Fort Ord, found levels of TCDD at 3.5 parts per trillion, more than double the remediation goal at the time of 1.2 ppt. Olson calls the evidence convincing. “It clearly supports the fact that 2,4,5-T with unknown amounts of dioxin TCDD was applied on the Fort Ord grounds and border fences,” Olson said. “Some military and civilian personnel would have been exposed.” The Department of Defense has described the Agent Orange used in Vietnam as a “tactical herbicide,” more concentrated than what was commercially available in the U.S. But Olson said his research suggests that even if the grounds maintenance crew used commercial versions of 2,4,5-T, which was available in the federal supply catalog, the soldiers would have been exposed to the dioxin TCDD. The half dozen veterans who spoke with KFF Health News said they want the military to take responsibility. The Pentagon did not respond to questions regarding the upkeep of the list or the process for adding locations. In the meantime, the Agency for Toxic Substances and Disease Registry is studying potential chemical exposure among people who worked and lived on Fort Ord between 1985 and 1994. However, the agency is evaluating drinking water for contaminants such as trichloroethylene and not contamination or pollution from other chemicals such as Agent Orange or those found in firefighting foams. Other veterans are frustrated by the VA’s long process to recognize their illnesses and believe they were sickened by exposure at Fort Ord. “Until Fort Ord is recognized by the VA as a presumptive site, it’s probably going to be a long, difficult struggle to get some kind of compensation,” said Mike Duris, a 72-year-old veteran diagnosed with prostate cancer four years ago who ultimately underwent surgery. Like so many others, he wonders about the connection to his training at Fort Ord in the early ’70s — drinking the contaminated water and marching, crawling, and digging holes in the dirt. “Often, where there is smoke, there’s fire,” Duris said. KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF. USE OUR CONTENTThis story can be republished for free (details). from https://ift.tt/B04pCrI Check out http://plush-draw15.tumblr.com/ Journalists Drill Down on Bird Flu Risks Opioid Settlement Payouts and Fluoride in Drinking Water4/27/2024 Céline Gounder, KFF Health News’ senior fellow and editor-at-large for public health, discussed the latest bird flu developments on CBS’ “CBS Mornings” on April 25. KFF Health News senior correspondent Aneri Pattani discussed the details of Tennessee’s distribution of $80 million in opioid settlement funds on WPLN’s “Morning Edition” on April 22.
KFF Health News contributor Andy Miller discussed water fluoridation on WUGA’s “The Georgia Health Report” on April 19.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF. USE OUR CONTENTThis story can be republished for free (details). from https://ift.tt/NRzdhBJ Check out http://plush-draw15.tumblr.com/ In the 2020 elections, then-candidate Joe Biden and many of his congressional colleagues loudly advocated for a federal “public option” health insurance plan. It was framed, at the time, as part of his incoming administration’s response to the pandemic. “Low-income Americans will be automatically enrolled in the public option at zero cost to them, though they may choose to opt out at any time,” Democrats promised in their party platform. But since Biden entered office, it’s been crickets. The president hasn’t uttered the phrase “public option” since December 2020, according to factba.se, which tracks his public remarks. Why the disappearing act? In a word: politics. “Out of the gate you’d have a huge powerful lobby against the public option — the hospitals — since providers have the most to lose: lots of money,” said Matthew Fiedler, an economist at the Brookings Institution who has studied payment disparities between insurance plans. The health-care industry is the largest lobbying sector in Washington, with more than$132 million spent annually just by hospitals and nursing homes, according to OpenSecrets. For those who’ve forgotten, the idea was to create a government-sponsored insurance plan to compete with commercial insurers under the Affordable Care Act. The concept, previously backed by President Barack Obama, didn’t make it into the final version of the ACA due to opposition from pretty much everyone in health care. In theory, a public option structured like Medicare, Medicaid or the military’s Tricare program could save billions in health-care spending by both the federal government and consumers because (like the existing federal plans) it would pay health providers less than commercial insurers. Fiedler said the public option could possibly save money, relative to commercial insurance, even if it paid as much as double Medicare’s rates. And without having to earn a profit, such a plan could spend more money on patient care. Unsurprisingly, insurers opposed the public option, but Fiedler said it’s hospital opposition that keeps it shelved. As an example, Fiedler points to Medicare drug price negotiation, another long shot Democratic priority. Biden got that across the finish line as part of his 2022 Inflation Reduction Act. “Congress didn’t want to pick a fight with hospitals, but they’re willing to take on drug companies,” Fiedler said. Biden’s party hasn’t yet put together its official platform for the 2024 election, so perhaps the public option will reappear on his agenda. Spokespeople for his reelection campaign and the White House didn’t respond to emailed questions about it. The idea still has many fans: Led by Colorado, some states have sought to create their own versions, though their plans rely on commercial insurers to administer the coverage. Insurers were able to tank public option proposals in Connecticut, and they’ve complained that they would lose money under Colorado’s proposal. This article is not available for syndication due to republishing restrictions. If you have questions about the availability of this or other content for republication, please contact [email protected]. KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF. USE OUR CONTENTThis story can be republished for free (details). from https://ift.tt/9LEaqRD Check out http://plush-draw15.tumblr.com/ Millions Were Booted From Medicaid. The Insurers That Run It Gained Medicaid Revenue Anyway.4/26/2024 Private Medicaid health plans lost millions of members in the past year as pandemic protections that prohibited states from dropping anyone from the government program expired. But despite Medicaid’s unwinding, as it’s known, at least two of the five largest publicly traded companies selling plans have continued to increase revenue from the program, according to their latest earnings reports. “It’s a very interesting paradox,” said Andy Schneider, a research professor at Georgetown University’s McCourt School of Public Policy, of plans’ Medicaid revenue increasing despite enrollment drops. Medicaid, the state-federal health program for low-income and disabled people, is administered by states. But most people enrolled in the program get their health care through insurers contracted by states, including UnitedHealthcare, Centene, and Molina. The companies persuaded states to pay them more money per Medicaid enrollee under the assumption that younger and healthier people were dropping out — presumably for Obamacare coverage or employer-based health insurance, or because they didn’t see the need to get coverage — leaving behind an older and sicker population to cover, their executives have told investors. Several of the companies reported that states have made midyear and retrospective changes in their payments to plans to account for the worsening health status of members. In an earnings call with analysts on April 25, Molina Healthcare CEO Joe Zubretsky said 19 states increased their payment rates this year to adjust for sicker Medicaid enrollees. “States have been very responsive,” Zubretsky said. “We couldn’t be more pleased with the way our state customers have responded to having rates be commensurate with normal cost trends and trends that have been influenced by the acuity shift.” Health plans have faced much uncertainty during the Medicaid unwinding, as states began reassessing enrollees’ eligibility and dropping those deemed no longer qualified or who lost coverage because of procedural errors. Before the unwinding, plans said they expected the overall risk profile of their members to go up because those remaining in the program would be sicker. UnitedHealthcare, Centene, and Molina had Medicaid revenue increases ranging from 3% to 18% in 2023, according to KFF. The two other large Medicaid insurers, Elevance and CVS Health, do not break out Medicaid-specific revenue. The Medicaid enrollment of the five companies collectively declined by about 10% from the end of March 2023 through the end of December 2023, from 44.2 million people to 39.9 million, KFF data shows. In the first quarter of 2024, UnitedHealth’s Medicaid revenue rose to $20.5 billion, up from $18.8 billion in the same quarter of 2023. Molina on April 24 reported nearly $7.5 billion in Medicaid revenue in the first quarter of 2024, up from $6.3 billion in the same quarter a year earlier. On April 26, Centene reported that its Medicaid enrollment fell 18.5% to 13.3 million in the first quarter of 2024 compared with the same period a year ago. The company’s Medicaid revenue dipped 3% to $22.2 billion. Unlike UnitedHealthcare, whose Medicaid enrollment fell to 7.7 million in March 2024 from 8.4 million a year prior, Molina’s Medicaid enrollment rose in the first quarter of 2024 to 5.1 million from 4.8 million in March 2023. Molina’s enrollment jump last year was partly a result of its having bought a Medicaid plan in Wisconsin and gained a new Medicaid contract in Iowa, the company said in its earnings news release. Molina added 1 million members because states were prohibited from terminating Medicaid coverage during the pandemic. The company has lost 550,000 of those people during the unwinding and expects to lose an additional 50,000 by June. About 90% of Molina Medicaid members have gone through the redetermination process, Zubretsky said. The corporate giants also offset the enrollment losses by getting more Medicaid money from states, which they use to pass on higher payments to certain facilities or providers, Schneider said. By holding the money temporarily, the companies can count these “directed payments” as revenue. Medicaid health plans were big winners during the pandemic after the federal government prohibited states from dropping people from the program, leading to a surge in enrollment to about 93 million Americans. States made efforts to limit health plans’ profits by clawing back some payments above certain thresholds, said Elizabeth Hinton, an associate director at KFF. But once the prohibition on dropping Medicaid enrollees was lifted last spring, the plans faced uncertainty. It was unclear how many people would lose coverage or when it would happen. Since the unwinding began, more than 20 million people have been dropped from the rolls. Medicaid enrollees’ health care costs were lower during the pandemic, and some states decided to exclude pandemic-era cost data as they considered how to set payment rates for 2024. That provided yet another win for the Medicaid health plans. Most states are expected to complete their Medicaid unwinding processes this year. KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF. USE OUR CONTENTThis story can be republished for free (details). from https://ift.tt/wJA4htN Check out http://plush-draw15.tumblr.com/ With little pomp, California launched two apps at the start of the year offering free behavioral health services to youths to help them cope with everything from living with anxiety to body acceptance. Through their phones, young people and some caregivers can meet BrightLife Kids and Soluna coaches, some who specialize in peer support or substance use disorders, for roughly 30-minute virtual counseling sessions that are best suited to those with more mild needs, typically those without a clinical diagnosis. The apps also feature self-directed activities, such as white noise sessions, guided breathing, and videos of ocean waves to help users relax. “We believe they’re going to have not just great impact, but wide impact across California, especially in places where maybe it’s not so easy to find an in-person behavioral health visit or the kind of coaching and supports that parents and young people need,” said Gov. Gavin Newsom’s health secretary, Mark Ghaly, during the Jan. 16 announcement. The apps represent one of the Democratic governor’s major forays into health technology and come with four-year contracts valued at $498 million. California is believed to be the first state to offer a mental health app with free coaching to all young residents, according to the Department of Health Care Services, which operates the program. However, the rollout has been slow. So slow that one of the companies has missed a deadline to make its app available on Android phones. Only about 15,000 of the state’s 12.6 million children and young adults have signed up for the apps, and school counselors say they’ve never heard of them. Advocates for youth question the wisdom of investing taxpayer dollars in two private companies. Social workers are concerned the companies’ coaches won’t properly identify youths who need referrals for clinical care. And the spending is drawing lawmaker scrutiny amid a state deficit pegged at as much as $73 billion. An App for That Newsom’s administration says the apps fill a need for young Californians and their families to access professional telehealth for free, in multiple languages, and outside of standard 9-to-5 hours. It’s part of Newsom’s sweeping $4.7 billion master plan for kids’ mental health, which was introduced in 2022 to increase access to mental health and substance use support services. In addition to launching virtual tools such as the teletherapy apps, the initiative is working to expand workforce capacity, especially in underserved areas. “The reality is that we are rarely 6 feet away from our devices,” said Sohil Sud, director of Newsom’s Children and Youth Behavioral Health Initiative. “The question is how we can leverage technology as a resource for all California youth and families, not in place of, but in addition to, other behavioral health services that are being developed and expanded.” The virtual platforms come amid rising depression and suicide rates among youth and a shortage of mental health providers. Nearly half of California youths from the ages of 12 to 17 report having recently struggled with mental health issues, with nearly a third experiencing serious psychological distress, according to a 2021 study by the UCLA Center for Health Policy Research. These rates are even higher for multiracial youths and those from low-income families. But those supporting youth mental health at the local level question whether the apps will move the needle on climbing depression and suicide rates. “It’s fair to applaud the state of California for aggressively seeking new tools,” said Alex Briscoe of California Children’s Trust, a statewide initiative that, along with more than 100 local partners, works to improve the social and emotional health of children. “We just don’t see it as fundamental. And we don’t believe the youth mental health crisis will be solved by technology projects built by a professional class who don’t share the lived experience of marginalized communities.” The apps, BrightLife Kids and Soluna, are operated by two companies: Brightline, a 5-year-old venture capital-backed startup; and Kooth, a London-based publicly traded company that has experience in the U.K. and has also signed on some schools in Kentucky and Pennsylvania and a health plan in Illinois. In the first five months of Kooth’s Pennsylvania pilot, 6% of students who had access to the app signed up. Brightline and Kooth represent a growing number of health tech firms seeking to profit in this space. They beat out dozens of other bidders including international consulting companies and other youth telehealth platforms that had already snapped up contracts in California. Although the service is intended to be free with no insurance requirement, Brightline’s app, BrightLife Kids, is folded into and only accessible through the company’s main app, which asks for insurance information and directs users to paid licensed counseling options alongside the free coaching. After KFF Health News questioned why the free coaching was advertised below paid options, Brightline reordered the page so that, even if a child has high-acuity needs, free coaching shows up first. The apps take an expansive view of behavioral health, making the tools available to all California youth under age 26 as well as caregivers of babies, toddlers, and children 12 and under. When KFF Health News asked to speak with an app user, Brightline connected a reporter with a mother whose 3-year-old daughter was learning to sleep on her own. ‘It’s Like Crickets’ Despite being months into the launch and having millions in marketing funds, the companies don’t have a definitive rollout timeline. Brightline said it hopes to have deployed teams across the state to present the tools in person by midyear. Kooth said developing a strategy to hit every school would be “the main focus for this calendar year.” “It’s a big state — 58 counties,” Bob McCullough of Kooth said. “It’ll take us a while to get to all of them.” Brightline’s contract states that the company was required to launch downloadable apps for iOS and Android phones by January, but so far BrightLife Kids is available only on Apple phones. Brightline said it’s aiming to launch the Android version over the summer. “Nobody’s really done anything like this at this magnitude, I think, in the U.S. before,” said Naomi Allen, a co-founder and the CEO of Brightline. “We’re very much in the early innings. We’re already learning a lot.” The contracts, obtained by KFF Health News through a records request, show the companies operating the two apps could earn as much as $498 million through the contract term, which ends in June 2027, months after Newsom is set to leave office. And the state is spending hundreds of millions more on Newsom’s virtual behavioral health strategy. The state said it aims to make the apps available long-term, depending on usage. The state said 15,000 people signed up in the first three months. When KFF Health News asked how many of those users actively engaged with the app, it declined to say, noting that data would be released this summer. KFF Health News reached out to nearly a dozen California mental health professionals and youths. None of them were aware of the apps. “I’m not hearing anything,” said Loretta Whitson, executive director of the California Association of School Counselors. “It’s like crickets.” Whitson said she doesn’t think the apps are on “anyone’s” radar in schools, and she doesn’t know of any schools that are actively advertising them. Brightline will be presenting its tool to the counselor association in May, but Whitson said the company didn’t reach out to plan the meeting; she did. 
Concern Over Referrals Whitson isn’t comfortable promoting the apps just yet. Although both companies said they have a clinical team on staff to assist, Whitson said she’s concerned that the coaches, who aren’t all licensed therapists, won’t have the training to detect when users need more help and refer them to clinical care. This sentiment was echoed by other school-based social workers, who also noted the apps’ duplicative nature — in some counties, like Los Angeles, youths can access free virtual counseling sessions through Hazel Health, a for-profit company. Nonprofits, too, have entered this space. For example, Teen Line, a peer-to-peer hotline operated by Southern California-based Didi Hirsch Mental Health Services, is free nationwide. While the state is also funneling money to the schools as part of Newsom’s master plan, students and school-based mental health professionals voiced confusion at the large app investment when, in many school districts, few in-person counseling roles exist, and in some cases are dwindling. Kelly Merchant, a student at College of the Desert in Palm Desert, noted that it can be hard to access in-person therapy at her school. She believes the community college, which has about 15,000 students, has only one full-time counselor and one part-time bilingual counselor. She and several students interviewed by KFF Health News said they appreciated having engaging content on their phone and the ability to speak to a coach, but all said they’d prefer in-person therapy. “There are a lot of people who are seeking therapy, and people close to me that I know. But their insurances are taking forever, and they’re on the waitlist,” Merchant said. “And, like, you’re seeing all these people struggle.” Fiscal conservatives question whether the money could be spent more effectively, like to bolster county efforts and existing youth behavioral health programs. Republican state Sen. Roger Niello, vice chair of the Senate Budget and Fiscal Review Committee, noted that California is forecasted to face deficits for the next three years, and taxpayer watchdogs worry the apps might cost even more in the long run. “What starts as a small financial commitment can become uncontrollable expenses down the road,” said Susan Shelley of the Howard Jarvis Taxpayers Association. This article was produced by KFF Health News, which publishes California Healthline, an editorially independent service of the California Health Care Foundation. KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF. USE OUR CONTENTThis story can be republished for free (details). from https://ift.tt/TVPiC7X Check out http://plush-draw15.tumblr.com/ The HostSome justices suggested the Supreme Court had said its piece on abortion law when it overturned Roe v. Wade in 2022. This term, however, the court has agreed to review another abortion case. At issue is whether a federal law requiring emergency care in hospitals overrides Idaho’s near-total abortion ban. A decision is expected by summer. Meanwhile, the Centers for Medicare & Medicaid finalized the first-ever minimum staffing requirements for nursing homes participating in the programs. But the industry argues that there are not enough workers to hire to meet the standards. This week’s panelists are Julie Rovner of KFF Health News, Joanne Kenen of the Johns Hopkins University’s nursing and public health schools and Politico Magazine, Tami Luhby of CNN, and Alice Miranda Ollstein of Politico. PanelistsAmong the takeaways from this week’s episode:
Plus for “extra credit” the panelists suggest health policy stories they read this week that they think you should read, too: Julie Rovner: NBC News’ “Women Are Less Likely To Die When Treated by Female Doctors, Study Suggests,” by Liz Szabo. Alice Miranda Ollstein: States Newsroom’s “Loss of Federal Protection in Idaho Spurs Pregnant Patients To Plan for Emergency Air Transport,” by Kelcie Moseley-Morris. Tami Luhby: The Associated Press’ “Mississippi Lawmakers Haggle Over Possible Medicaid Expansion as Their Legislative Session Nears End,” by Emily Wagster Pettus. Joanne Kenen: States Newsroom’s “Missouri Prison Agency To Pay $60K for Sunshine Law Violations Over Inmate Death Records,” by Rudi Keller. Also mentioned on this week’s podcast:
CreditsFrancis Ying Audio producer Emmarie Huetteman EditorTo hear all our podcasts, click here. And subscribe to KFF Health News’ “What the Health?” on Spotify, Apple Podcasts, Pocket Casts, or wherever you listen to podcasts. KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF. USE OUR CONTENTThis story can be republished for free (details). from https://ift.tt/gMYSJcr Check out http://plush-draw15.tumblr.com/ The Biden administration wants to make it easier for Americans to get dental care. But don’t try booking an appointment just yet. A new regulation out this month allows states to include adult dental care as a benefit that health insurers must cover under the Affordable Care Act. Following record ACA enrollment this year, the proposal represents an election-year aspiration for the future of Obamacare: It doesn’t require states to do anything, even as it shows off President Biden’s intention to make the ACA a more robust safety net. “It’s huge, really significant,” said Colin Reusch, director of policy at Community Catalyst, a health coverage advocacy group. He said the new Biden administration rule represents “one of the first real changes” to coverage provisions of the law since it passed in 2010. But like so much in health care, expanding access to dental services is a lot more complicated than it sounds. An estimated 68.5 million U.S. adults lacked dental insurance in 2023, according to the nonprofit CareQuest Institute for Oral Health. That’s more than 2.5 times the roughly 26 million Americans of all ages who lack health insurance. And millions of Americans lost dental coverage in the past year as part of the Medicaid “unwinding” that dropped low-income people who had been covered by the program during the pandemic. At the same time, untreated dental disease is estimated to cost the United States more than $45 billion in lost productivity annually, according to the Centers for Disease Control and Prevention, and it’s linked to a long list of even more serious health problems, including heart disease and diabetes. Still, efforts to expand U.S. dental coverage have long foundered on the shoals of cost. When people have dental insurance, they tend to use it. So including the coverage in a health insurance policy can raise overall premiums. That’s one reason traditional Medicare coverage explicitly excludes most dental care. (Many private Medicare Advantage plans offer some dental coverage as an enticement for seniors to join.) An effort to add a dental benefit to Medicare was stripped from Biden’s “Build Back Better” legislation before it was passed in 2022 as the Inflation Reduction Act. Instead, the administration clarified and expanded the limited circumstances in which Medicare can cover dental care. Any progress on oral health — including giving states the option to require coverage for adults — is seen by advocates as a victory. Dental coverage for children is already an essential benefit under the ACA. But whether they actually get coverage depends on states affirmatively adding dental benefits to benchmark plans in the ACA’s insurance marketplaces. Those plans not only determine what services Affordable Care Act insurance has to cover, but also set parameters for state-employee and many private-employer health plans. Reusch said a few states are considering the change, but it will be a while until anything is certain. States have until May 2025 to decide whether to add dental care to benchmark ACA plans; the benefit wouldn’t be effective until the 2027 plan year. This article is not available for syndication due to republishing restrictions. If you have questions about the availability of this or other content for republication, please contact [email protected]. KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF. USE OUR CONTENTThis story can be republished for free (details). from https://ift.tt/BY7zDyK Check out http://plush-draw15.tumblr.com/ |
 RSS Feed
RSS Feed
